Spotlight 5
The impacts of isolation
More than 500 complaints about restrictions on visitation were reported, mostly arising from the COVID-19 pandemic.
How do we find the right balance?
Background
In years 4 and 5, Patient Ombudsman received more than 500 complaints about restrictions on visitation including 269 complaints about public hospitals, 206 about long-term care homes, and 31 about other residential care settings that are outside of Patient Ombudsman’s jurisdiction. Ninety-six percent of the complaints occurred between March 2020 and March 2021 and involved visitation restrictions arising from the COVID-19 pandemic.
Monthly complaints about visitation by health sector
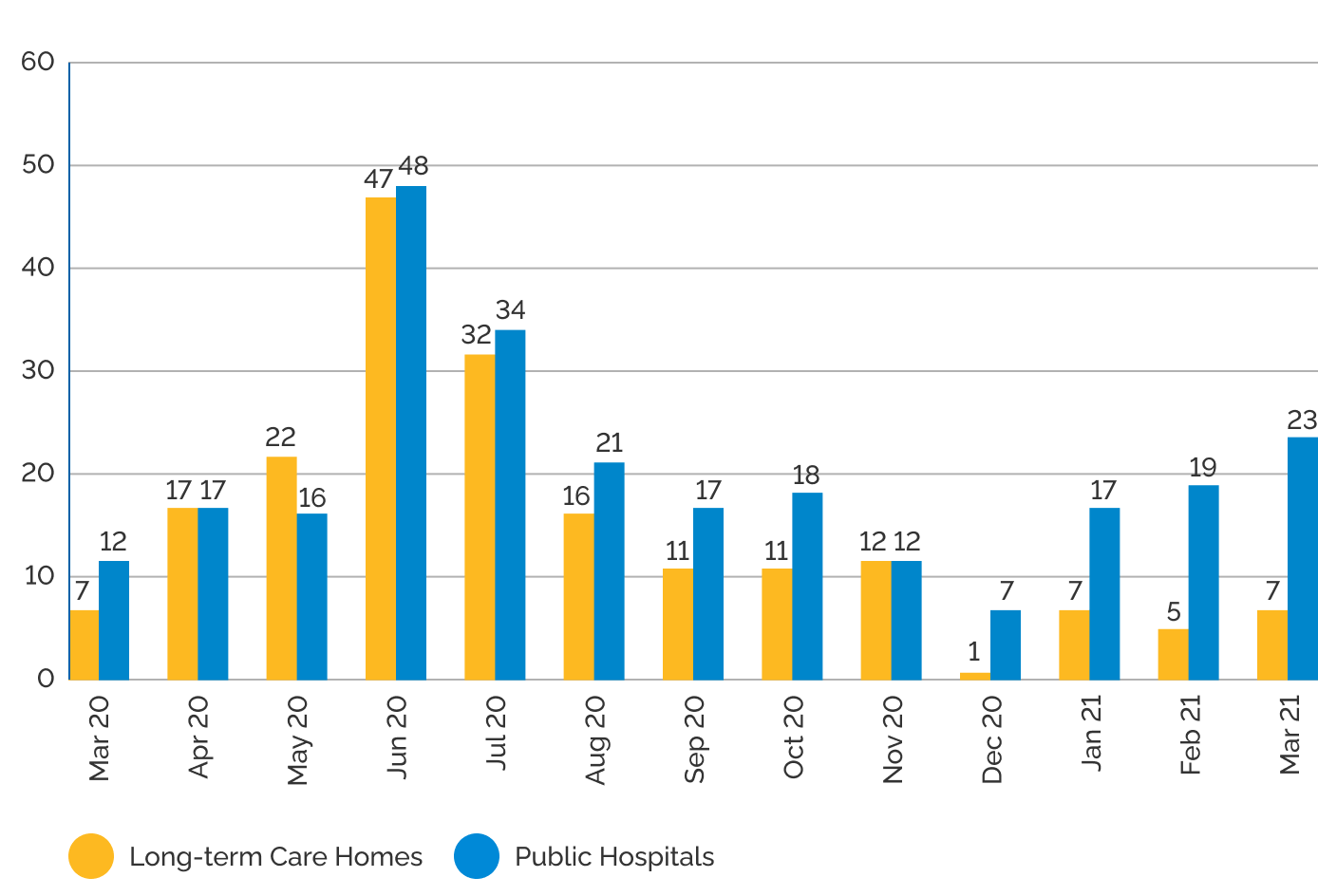
As shown in the "Monthly complaints about visitation by health sector" chart, complaints about visitation restrictions in long-term care homes peaked in the summer of 2020 and have continued, but with less frequency since December 2020. In the latter part of year 5, complaints about visitation in long-term care homes most often involved confusion about changes to policy guidance over time, miscommunication and reports about homes that implemented visitor policies that were more restrictive than suggested by the provincial guidance.
Patient Ombudsman has highlighted the effects of visitation restrictions on long-term care home residents in its three special reports on COVID-19. The complaints received by Patient Ombudsman over the course of the pandemic and the results of Patient Ombudsman’s public survey describe the impacts of isolation, lack of stimulation and absence of support from family caregivers on the health and well-being of many long-term care home residents.
The Government of Ontario has recognized the importance of visitation and provided specific guidance to long-term care homes, including the requirement for homes to have policies on visitation that reflect government directives and guiding principles:
Safety
Any approach to visiting must balance the health and safety needs of residents, staff and visitors and ensure risks are mitigated
Emotional well-being
Welcoming visitors is intended to support the mental and emotional well-being of residents by reducing any potential negative impacts related to social isolation
Equitable access
All residents must be given equitable access to receive visitors, consistent with their preferences and within reasonable restrictions that safeguard residents
Flexibility
The physical or infrastructure characteristics of the home, its workforce or human resources availability, whether the home is in an outbreak and the current status of the home with respect to personal protective equipment (PPE) are all variables to consider when setting home-specific policies
Equality
Residents have the right to choose their visitors. In addition, residents or their substitute decision-makers have the right to designate caregivers
Public hospitals have received less specific provincial guidance on visitation. In June 2020, the Ministry of Health’s guidance for acute care was amended to recognize the importance of visitors to patients’ well-being. The guidance urged hospitals to be adaptive and flexible and balance the need to mitigate risks with “the mental, physical and spiritual needs of patients for their quality of life.” Complaints to Patient Ombudsman about visitation in hospitals have remained relatively high into 2021.
It’s not unusual for public hospitals to have visitor policies that vary by unit or site based on the judgment and decisions of individual unit managers. This can be confusing and frustrating for visitors who may have limited access to information about the reasons for varying policies and rules.
Patient Ombudsman continues to recommend that all HSOs should adopt the least restrictive limits on visitation based on risks and evidence, and that policies should be clearly communicated to those affected and provide for exceptions on compassionate grounds.
While there may be valid reasons for different units in hospitals to have different policies based on the risks to patients, the availability of staff resources or other factors, it serves no one if the policies appear to be arbitrary or cannot be explained to patients and caregivers. The decisions of unit managers should be based on a consistent framework with guiding principles that ensure fairness and transparency and recognize the importance of a least restrictive approach.
Resources
- Essential Care Partner and Visitor Presence Policies and Resources, Ontario Hospital Association, September 2021.
- Honouring the voices and experiences of Long-Term Care Home residents, caregivers and staff during the first wave of COVID-19 in Ontario: Special Report, Patient Ombudsman, October 2020.
- Honouring Voices and Experiences Reflections from waves 2 and 3 of the pandemic: Special Report 2, Patient Ombudsman, August 2021.
- Honouring Voices and Experiences – Long-term care home survey: Special Report 3, Patient Ombudsman, December 2021.
- COVID-19 Guidance: Acute care, Version 6, Ministry of Health, June 15, 2020.
- COVID-19 guidance document for long-term care homes in Ontario, Government of Ontario, published May 4, 2021, most recent update December 14, 2021.